



The Clinical Partnership Problem: How MedTech AI Startups Can Get Hospital Data Without Giving Away the Company


Every healthcare AI startup needs hospital data. Every hospital has data they might share. The gap between those two facts is six to eighteen months of negotiation, legal review, ethics approval, and governance process — if the partnership succeeds at all.
Most founders underestimate this gap. They assume that a convincing clinical use case and a credible team is enough to unlock a hospital data partnership. It's necessary but not sufficient. Hospitals have data governance frameworks, legal constraints, and institutional incentives that operate independently of clinical interest in your technology.
This article covers what clinical data partnerships actually involve — the legal, governance, and commercial structure — and how to negotiate them in a way that gives you the data you need without terms that compromise your company's long-term position.
Companion piece to our health AI series: the data problem in healthcare AI for the strategies you use when partnerships aren't available; clinical validation for the evidence package the partnership data has to support; SaMD classification for whether your product is regulated as a medical device; and AI in women's health for partnership dynamics in particularly sensitive clinical domains.
Why Hospitals Are Cautious About Data Partnerships
Before approaching a hospital for a data partnership, understanding their position is essential.
Legal liability is real. A hospital that shares patient data with a commercial entity for AI development faces liability under UK GDPR / EU GDPR, the Data Protection Act, and potentially NHS-specific data governance frameworks (for UK trusts). If the data is misused, inadequately secured, or shared in violation of consent conditions, the hospital bears regulatory and reputational consequences — not just the startup.
Institutional incentives don't align by default. Hospital clinicians and research teams may be genuinely enthusiastic about your technology. Hospital legal and information governance teams — who must review and approve any data sharing agreement — are optimised for risk minimisation, not partnership speed. These are different functions with different incentives, and the decision requires sign-off from both.
Data has value that hospitals are increasingly aware of. The narrative around patient data as a strategic asset has reached hospital boardrooms. NHS trusts, in particular, are increasingly aware that their data — especially imaging data and longitudinal EHR data — has significant commercial value, and they are less willing than they were five years ago to share it for minimal return in exchange for "collaboration."
Research governance adds additional cycles. If your data use involves research (as opposed to purely operational purposes), NHS trusts require Research and Innovation approval, which involves an R&I department review. Studies involving patient data typically also require Research Ethics Committee (REC) approval, which adds a further review cycle with its own committee timelines.
Understanding these constraints before your first meeting with a hospital partner is what allows you to structure the conversation realistically.
The Legal Basis Question: Get This Right First
Under UK GDPR and EU GDPR, processing special category health data — which is what clinical data is — requires both a lawful basis under Article 6 and a specific condition under Article 9. Getting the legal basis analysis right before approaching a hospital is essential — hospitals' legal and IG teams will ask, and the answer determines the structure of the entire partnership.
For model training and development (commercial purpose)
The lawful basis options under Article 6 include: legitimate interests (Article 6(1)(f)), performance of a task in the public interest (Article 6(1)(e)), and consent (Article 6(1)(a)). For commercial model development by a private company, legitimate interests is the most commonly applicable basis — but it requires a balancing test demonstrating that the company's legitimate interest in using the data outweighs the data subjects' interest in privacy. This analysis needs to be documented.
Under Article 9, the special category conditions applicable to medical AI development include: scientific research (Article 9(2)(j)) with appropriate safeguards, and explicit consent (Article 9(2)(a)).
The practical implication: commercial AI model development on identifiable patient data is legally complex. Most partnerships either use pseudonymised data (reducing GDPR risk, though not eliminating it for data that could be re-identified), obtain explicit patient consent (ethically most robust but operationally very expensive), or structure the work under a research exemption (Article 89) with appropriate research governance.
For direct patient care (operational purpose)
If your AI system is being used in a clinical pilot to support direct patient care — not for model training — the legal basis is cleaner: Article 9(2)(h) (processing necessary for provision of health care) typically applies, with GDPR Article 6(1)(c) (legal obligation) or 6(1)(e) (public interest task) as the Article 6 basis. This is why clinical pilots with NHS trusts often proceed faster than research data partnerships — the legal framework for direct care use is better established.
The US / HIPAA parallel
The US framework is different in detail but structurally similar. Hospitals operate as HIPAA covered entities; AI startups receiving patient data act as business associates under a Business Associate Agreement (BAA) that specifies permitted uses, security obligations, and breach reporting. Research use of patient data typically requires Institutional Review Board (IRB) approval, the equivalent of UK REC review. State-level reproductive health data restrictions (Washington's My Health My Data Act, California's CMIA, others) add additional layers post-Dobbs. The three partnership models below translate broadly to US deployments with HIPAA-specific structural changes.
The Three Partnership Models
Clinical data partnerships take three main structural forms, with different legal and commercial implications.
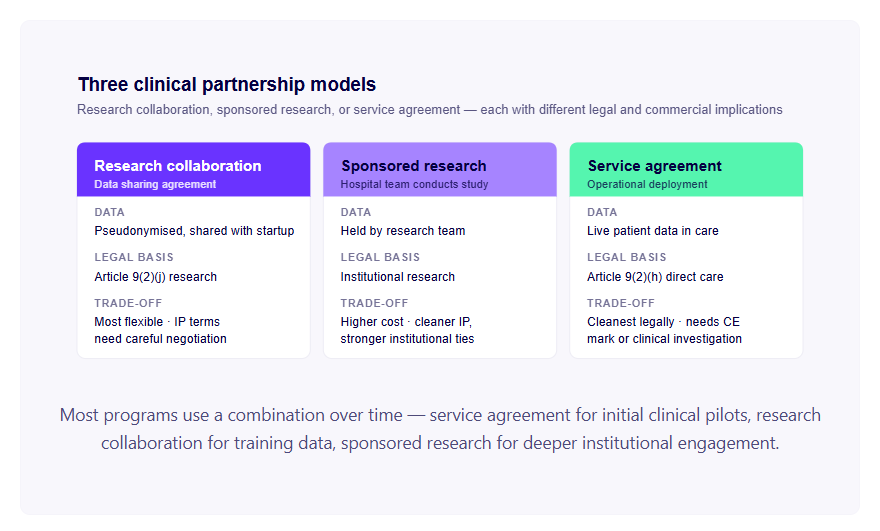
Model 1: Research collaboration with data access. The startup enters a research collaboration agreement with the hospital. The hospital provides access to pseudonymised patient data under a formal data sharing agreement. Processing is conducted under Article 9(2)(j) research exemption with appropriate safeguards (pseudonymisation, purpose limitation, data minimisation). The collaboration may be supported by a Research Ethics Committee application and NHS R&I approval.
Commercial terms to negotiate: Who owns the trained model? What rights does the hospital have to use the AI system developed from their data? Does the hospital receive equity, revenue sharing, or a perpetual licence? Is the collaboration exclusive or non-exclusive?
The common trap: hospitals requesting equity stakes or revenue sharing for data partnerships. Equity for data is rarely the right commercial structure for a startup — it creates a messy cap table and doesn't reflect the hospital's actual commercial contribution. Revenue sharing on a percentage of future revenue from the trained model is a more common and more defensible structure, but only if the hospital's data is genuinely central to the model's commercial value.
Model 2: Sponsored research agreement. The startup funds a hospital research team to conduct a defined research study using the hospital's patient data. The research team conducts the study, publishes results, and provides the startup with the trained model or the training dataset under defined conditions. Intellectual property terms are specified in advance.
Commercial terms to negotiate: IP ownership (typically negotiated between the startup's preference for full IP ownership and the hospital's preference for a royalty-free research licence), publication rights (hospitals need to publish for research mission reasons; startups may want to embargo publications until patent applications are filed), exclusivity (does the research team work exclusively with the startup on this topic, or can they work with competitors?).
This model is slower and more expensive than Model 1 (you're paying for the research staff's time), but it provides cleaner IP ownership and involves the hospital's research team in a way that creates stronger institutional relationships.
Model 3: Service agreement with data processing. The startup provides an AI service to the hospital — model inference on the hospital's patient data — under a services agreement. The hospital's data is processed as part of service delivery, under the hospital's Article 9(2)(h) direct care basis. The startup receives inference fees and, depending on the agreement, the right to use non-identifiable outputs for model improvement.
This is the cleanest commercial structure from a GDPR perspective (direct care processing is less legally complex than research processing) but it requires the AI service to be deployable in a clinical setting — which requires either CE marking or a formal clinical investigation agreement.
Data Sharing Agreement Terms You Must Negotiate
Regardless of which partnership model you use, the data sharing agreement will contain terms that significantly affect your company's commercial and technical position. These are the terms to negotiate carefully.
Purpose limitation. The agreement will specify the permitted purposes for which the shared data can be used. Most hospitals will want purpose limitation to the specific stated purpose — model training for Indication X — with any extension of use requiring a new agreement or amendment. This is reasonable, but the definition of "purpose" should be broad enough to cover the full intended scope of model development — training, validation, testing, and model improvement — not just initial model training.
Data minimisation. The agreement will require that only the minimum data necessary for the stated purpose is processed. For AI model training, this needs to include all clinical variables that are candidate features for the model — a broader set than you may ultimately use. Defining the required dataset schema before the agreement is signed avoids the need for amendments when the data scientists identify additional variables they need.
IP ownership. The default position of most hospital legal teams is that IP developed using their data should be jointly owned or subject to a royalty-free licence to the hospital. For a startup, joint IP ownership is problematic — it limits your ability to license, sell, or enforce the IP without the hospital's consent. The preferred position for a startup is full IP ownership with a perpetual, royalty-free, non-commercial licence back to the hospital for use in their clinical practice.
Publication and confidentiality. Hospitals and academic medical centres need to be able to publish research results — it's a requirement for funding and for academic staff career progression. The startup needs time to protect IP before publication. The standard negotiated position: the startup has a 30–90 day review window before publication to identify patentable content and request delays; the hospital can publish after the review window without the startup's approval.
Data retention and deletion. The agreement will specify how long the startup can retain the shared data and what happens to it at the end of the agreement. "Delete and certify deletion within 30 days of agreement termination" is standard. For a startup, this means that trained model weights — which don't contain patient data — are separately owned and not subject to deletion, but the training dataset itself must be deleted on schedule.
Audit rights. Hospitals may include audit rights — the right to inspect how the startup is using the data, what security controls are in place, and whether the agreement terms are being followed. Reasonable audit rights with defined notice periods (30 days) and frequency limits (once per year) are standard. Unlimited audit rights with no notice period are not reasonable to accept.
The EU AI Act and EHDS Overlays
Two regulatory frameworks now sit on top of GDPR for clinical data partnerships in 2026.
EU AI Act training data governance (Article 10). For AI medical device software classified as high-risk (Class IIa+ under MDR/IVDR is automatically high-risk under the AI Act), the AI Act imposes specific training data governance requirements that affect partnership structuring. Training data must be documented as relevant, representative, and free of obvious errors for the intended use; data quality, subgroup composition, and bias testing must be documented. These requirements affect what data you need from your hospital partner, what the data documentation must include, and what evidence you need to retain for the AI Act conformity assessment. Build these documentation requirements into the partnership agreement from the start — retrofitting them is significantly harder.
European Health Data Space (EHDS). The EHDS regulation, in force from 2025, creates a harmonised framework for secondary use of health data across EU member states. EHDS designates health data access bodies in each member state and creates a structured process for requesting access to multi-country data for research, AI development, and other secondary uses. Implementation is gradual through 2025–2028, but the framework is increasingly relevant for clinical AI programs with multi-country EU ambitions. For partnerships in 2026 and beyond, EHDS provides a more structured route for cross-border data access than country-by-country negotiation, and partnerships designed against EHDS frameworks now will be better positioned as implementation matures.
Practical Strategies for Accelerating Clinical Partnerships
Start with a pilot, not a partnership. A clinical evaluation agreement — using the AI system in clinical practice to evaluate its utility — is faster to negotiate than a data sharing agreement for model training. The legal basis for clinical evaluation is cleaner (direct care processing), the governance requirements are lower, and a successful pilot creates the institutional buy-in needed to negotiate a deeper data partnership from a position of demonstrated clinical value.
Identify a clinical champion before engaging IG and legal. Hospital partnership negotiations move at the speed of the slowest reviewer. A senior clinician who is genuinely enthusiastic about your technology, who understands the hospital's internal governance processes, and who is willing to advocate internally for the partnership is worth more than any amount of external pressure or relationship building with procurement.
Use existing research frameworks where possible. NHS trusts that are part of Academic Health Science Networks (AHSNs) or NIHR (National Institute for Health and Care Research) Clinical Research Networks have established data access frameworks and experienced R&I teams. Approaching through these frameworks — rather than directly to the trust's information governance team — can significantly reduce timeline. Similarly, NHS DigiTrials (for recruitment and data access support) and HDR UK (for access to multi-site health datasets) have established legal and governance frameworks that avoid starting from scratch.
Get your own governance in order before approaching hospitals. Hospitals' IG teams will ask about your GDPR compliance, your data security controls, your Cyber Essentials certification, your data processor agreements with your cloud providers, and your technical and organisational measures for protecting patient data. Being unable to answer these questions delays the partnership. Having documented, credible answers accelerates it.
The startups that close clinical partnerships fastest aren't the ones with the most compelling technology. They're the ones whose own data governance is credible enough that the hospital's IG team can complete their review without raising substantial concerns.
Where Vector Labs Fits
Vector Labs has navigated NHS and EU hospital data partnerships for clinical AI development, including work with NHS-partnered women's health applications. We work with healthcare AI founders at three points: partnership scoping (legal basis analysis, model selection, commercial term strategy), governance and documentation (data sharing agreements, DPIA, R&I and ethics applications, AI Act training data documentation), and execution (multi-site framework navigation, federated infrastructure where appropriate, ongoing partner relationship management).
If you're planning a clinical partnership and want to understand the legal and commercial structure before your first hospital meeting, get in touch at vector-labs.ai.
For the broader series: the data problem in healthcare AI covers strategies when partnerships aren't available; clinical validation covers the evidence package the partnership data has to support; SaMD classification covers whether your product is regulated as a medical device; and AI in women's health covers partnership dynamics in particularly sensitive clinical domains.
FAQs
For a research-purpose data sharing agreement with a single NHS trust, expect 6–12 months from initial contact to signed agreement and data flow. The bottleneck is usually the trust's Information Governance team review, R&I approval, and ethics review (if required) running in sequence rather than in parallel. Trusts with experienced IG teams and established frameworks for AI partnerships move faster (3–6 months). Trusts with new IG infrastructure or no prior AI partnership experience can take 12–18 months.
Generally no. Equity for data creates a messy cap table, doesn't reflect the hospital's actual commercial contribution to your product, and creates governance complications when the hospital is also a customer or potential customer. Revenue sharing on a defined percentage of future revenue tied to models trained on the partner's data is a more defensible structure. Royalty-free licence-back for the hospital's own clinical use is often acceptable as additional consideration.
Under GDPR, anonymised data is data from which the data subject cannot be identified by any reasonably likely means — and is therefore outside GDPR scope. Pseudonymised data is data where direct identifiers have been replaced with a key (which is held separately), but the data could be re-identified with access to that key — and remains within GDPR scope. Most clinical AI training uses pseudonymised rather than truly anonymised data because true anonymisation of clinical data is hard to achieve while preserving training utility.
Yes, with the right legal basis and governance structure. The most common path is a research collaboration under Article 9(2)(j) (scientific research) with Article 89(1) safeguards — pseudonymisation, purpose limitation, data minimisation, and appropriate institutional review. Commercial purpose is permitted under this framework, but it triggers careful balancing test analysis and typically requires R&I and ethics approval. NHS trusts vary in how comfortable they are with explicitly commercial purposes; trusts with strong AHSN involvement are typically easier.
For research that involves NHS patient data, typically yes — Research Ethics Committee approval is required for the research study under which the data is shared. Approval timelines vary: NHS HRA (Health Research Authority) approval for an integrated research application typically takes 60–90 days. For studies using only previously collected, de-identified data, a Confidentiality Advisory Group (CAG) approval may be required instead of full REC review. Plan ethics review into your timeline from the beginning.
Three patterns that work. First, royalty-free perpetual licence to the hospital for use of the developed AI in their clinical practice, plus the startup retains full IP ownership. Second, single-digit revenue share (1–5%) on revenue specifically generated from products trained on the partner's data, capped at a defined amount or duration. Third, fixed-fee research collaboration where the hospital is paid for the work (research team time, data preparation, governance support) and the startup retains IP. Equity stakes for data are rarely the right structure.
Multi-site partnerships compound complexity. Each trust has its own IG processes, R&I procedures, and contracting timelines. Practical approaches: use a federated data infrastructure where data doesn't leave each trust (federated learning, distributed querying); engage through an aggregator framework like HDR UK or an NIHR network that has multi-site governance pre-established; or sequence the trusts, starting with one as the lead trust and using their approval as a reference for subsequent trusts. Plan multi-site partnerships at 12–24 months minimum.
The European Health Data Space (EHDS), in force from 2025, creates a harmonised framework for secondary use of health data across EU member states. For health data sharing across borders, EHDS provides a more structured route than the current country-by-country approach. For clinical AI startups, EHDS is becoming a meaningful path for accessing multi-country training data. The implementation is gradual through 2025–2028; first applications are emerging now for research use cases. Worth designing for if your AI program has multi-country EU ambitions.